


-
 BABY BOOMERS
BABY BOOMERSBaby Boomer Aging Statistics Are Staggering [VIDEO]
-
 ADVERTISING
ADVERTISINGBaby Boomers are STILL the Largest Consumer Group in America
-
 BABY BOOMERS
BABY BOOMERSBaby Boomers Have 10,000 Days to Change the World [Book/Video]
-
 BABY BOOMERS
BABY BOOMERSBoomerang Kids Can Jeopardize Baby Boomers’ Retirement Plans [VIDEO]
-
 BABY BOOMERS
BABY BOOMERSThe Influence of the Baby Boomer Generation
-
 BABY BOOMERS
BABY BOOMERSTHE ROCK STAR CHRONICLES Interviewing The Legends by Ray Shasho [BOOK]
-
 BABY BOOMERS
BABY BOOMERSBaby Boomer Generation is Financially Optimistic
-
 BABY BOOMERS
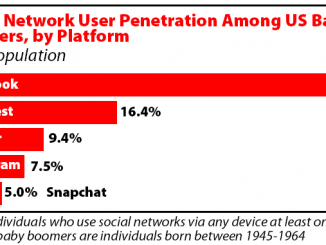
BABY BOOMERSSocial Networking for Baby Boomers by Dotsie Bregel
-
 BABY BOOMERS
BABY BOOMERSBoomers Getting Married Again Need to Discuss Finances Before the Wedding
-
 BABY BOOMERS
BABY BOOMERSBaby Boomers Want to do it ‘Our Way’ [VIDEO]











-
 Boomer Surveys-Questionnaires-Polls
Boomer Surveys-Questionnaires-PollsPOLITICAL – SURVEYS-QUESTIONNAIRES-POLLS
-
 Boomer Surveys-Questionnaires-Polls
Boomer Surveys-Questionnaires-PollsSurveys/Polls – POLITICAL
-
 BABY BOOMERS
BABY BOOMERSSurveys/Polls – Economic
-
 BOOMER RETIREMENT
BOOMER RETIREMENTSurveys-Questionnaires-Polls – Retirement Locations